


Empowered Patients and the Transformation of Healthcare Ecosystems

The COVID-19 pandemic has broken down the competitive barriers between traditional providers and digital healthcare delivery companies. For example, digital first companies such as Teladoc and Doctor Care Anywhere are gaining traction with national payers and private insurance providers in the UK and US to provide subscriptions to different services, primarily in primary care. The same is true for Ping An Good Doctor in China. Interestingly, Ping An started connecting healthcare providers and patients through health insurance before eventually enabling doctors external to affiliated providers to consult patients remotely, offering a wide range of virtual health services. They more recently provided application programming interfaces (API) to third-party developers to add complementary services for providers, doctors and patients including applications for AI-enabled radiology and pathology, but also mobile payments. Ping An Good Doctor is China’s largest digital healthcare platform, with more than 200 million users and collaborating with over 3,000 hospitals to provide services such as hospital referrals, appointments, and inpatient arrangements.
But the COVID-19 pandemic is not the sole disruptive force to transforming healthcare ecosystems.
In the last two decades or so, there has been increasing pressure toward personalized or precision medicine from healthcare providers, doctors, patients and even payers. These pressures have been institutionalized in new policies and have had ripple effects across other ecosystem actors such as pharmaceutical and biotech organizations as well as medical device manufacturers. Personalized medicine is the targeted process of administering the most appropriate treatment for an individual patient at the most appropriate time and with the correct dose.
Others have extended this notion of precision medicine as the need to shift our mindset to a focus on preventing disease as opposed to simply treating disease. The key objective is to handle each patient as a unique individual away from the current one-size-fits-all, trial-and-error approach that characterizes most healthcare practices today. Personalized medicine uses molecular diagnostic tools to identify specific biological markers, including genetic and physiological, to help assess methods of preventing disease as opposed to treating it after the fact. By combining the data from these tests with a patient's medical history and personal circumstances, health care providers can develop targeted prevention plans first and foremost. This goal toward preventing disease is also linked to continued efforts by healthcare systems around the globe to have zero patient encounters – to avoid expensive diagnostic and treatment practices in hospitals. The use of wearables, home monitoring and other sensor technologies aim to achieve this goal and feed into the need toward personalized medicine. Patients want to be able to manage their own health and wellness, on demand, at the comfort of their own home with smart technologies.
First, there is demand for safer and more effective treatment options. To give an example, data has shown that major drugs such as hypertension drugs like ACE, and heart failure drugs such as beta blockers have varied effectiveness across different patients, while the side effects also vary. If we extrapolate for those inefficiencies where drugs do not work to the cost of ineffectiveness to the healthcare system a lot of money could be saved and reinvested in more targeted prevention and treatment plans. In fact, ineffective therapies can cause harmful side effects that can further increase the costs to the healthcare system.
Some studies have shown that between 7-15% of hospital admissions are linked to adverse drug reactions. There are hundreds of thousands of deaths per year from such adverse drug reactions, and many patients experience adverse drug reactions during hospital stay. Thus, both the financial costs, but also the cost of human lives is high when following more traditional, population-level health prevention and treatment plans where the focus is on how specific treatments work on average across a population segment. Clinical trials on effective drug treatments “take heterogeneous inputs (the people in the study or studies) and come up with homogeneous results (the average result across all those people). Evidence-based medicine then insists that we apply those average findings back to individuals. The problem is that no patient is strictly average”.
In contrast, precision medicine can provide more tailored, personalized healthcare plans, especially in the case of chronic conditions, as well as conditions based on genetic markers. The key objective is to assess the risk of following plan A as opposed to plan B not for the average individual in the population segment, but rather in relation to the unique mix of symptoms and risk factors for a specific patient. Such a personalized approach would weigh the risk versus reward versus cost of therapy for individual patients while paying more attention to maintaining the quality of life for a longer period of time.
Second, personalized medicine is driven by recent advances in biotechnologies, especially whole genome sequencing. Whole genome sequencing offers the ability to identify rare variants in genetic disorders enabling a better understanding and management of rare and chronic diseases. The first sequence of the human genome was completed in 2003 and cost approximately $150 million. Since then, the cost of whole genome sequencing has dropped from $14000 in 2006 to $1000 in 2015. Today the cost is somewhere in between $500-1000. This drop in cost, is closely aligned with faster computing processors, improved data storage and nanotechnology, as well as advancements in genomics and molecular technologies. But it is not just the cost that has dropped, it is also the speed by which human genome sequence can be done. From a timeline of 6 to 8 years, some companies like Illumina are now able to do multiple whole genome sequences in a day. And finally, from big laboratories where human genome sequencing could previously be done, we are now in an era where portable devices are used to do the genome sequencing.
Whole genome sequencing is a disruptive technology that is further driving transformation toward personalized medicine. Whole genome sequencing can help explain how patients with the same disease exhibit different medical trajectories, while reacting differently to treatment plans. Although all human beings are 99.8% identical, we each have about three to five million differences in our genome compared to another person. Certainly, most of those differences are common variants, they exist in a few percent in the population. Only a very small fraction of those variants is relatively rare. Whole genome sequencing enables an identification of the risks involved for getting a disease if a variant is present, as well as which of those variants may protect us from getting the disease.
In the UK, the 100,000 Genomes Project, sequenced the genomes of 100,000 individuals affected by a rare disease, or cancer. Approximately 6 to 7 percent of the UK population is affected by cancer or a rare disease each year. Cancer begins because of changes in genes within what was a normal cell. Although a cancer starts with the same DNA as the patient, it develops mutations or changes which enable the tumour to grow and spread. By taking DNA from the tumour and DNA from the patient’s normal cells and comparing them, the 100,000 Genomes Project was able to detect the precise changes in a patient’s cells. This pilot project has now been transformed to routine genomics services on rare and chronic diseases provided by Genomics England, a wholly owned subsidiary of the Department of Health & Social Care. Knowing and understanding these changes strongly indicates which treatments will be the most effective. Genomics has already started to guide and inform doctors about the best treatment for individual patients or their relatives. Knowledge of the whole genome sequence may identify the cause of chronic and rare diseases and help point the way to new methods of preventing these diseases, as well as learning to live with them while managing the risks involved. As most rare diseases are inherited, the genomes of the affected individual (usually a child) plus two of their closest blood relatives are included to pinpoint the cause of the condition. Acting early to identify the genomic and biological markers of a disease – as early as birth – can help an individual prevent disease. Changing nutritional and exercise patterns on the basis of such as, genomic and biological markers, can help individuals avoid the onset of negative consequences such as falling victims of the metabolic syndrome that can spiral genetic disease out of control much earlier than otherwise.
Beyond national initiatives like the 100,000 Genomes Project, there are also many private initiatives. One example is Human Longevity, a facility that enables individuals to having their genome sequenced, to then predict the probability that they will develop a disease or to suffer from a medical condition such as heart failure in the future. Human Longevity combines a large database of genomic and phenotypic data with imaging data and machine learning to drive discoveries and deliver curated personal health information. The scientists at Human Longevity published the results of a three-year study that enrolled 1190 presumed healthy participants aged 18 and above. To the surprise of the participants, 86% of them were found to be genetic carriers of recessive diseases such as Alzheimer’s and 24% of them were found to have a rare genetic mutation that will affect their health in the future. A total of 206 unique medically significant variants in 111 genes were identified. These are shocking findings with potentially life-changing outcomes, especially for the higher risk participants, who after this study were recommended to undergo additional tests, and to enroll in preventative measures to manage their health risk.
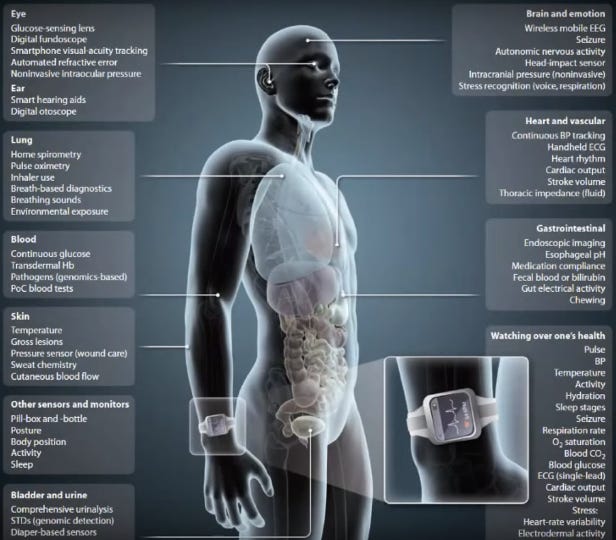
Third, whole genome sequencing, together with other technologies such as medical imaging, biosensors and machine learning algorithms that detect patterns in the data are significantly augmenting medical decision making, while empowering patients to take a more active role in the management of their health and wellness. Empowered patients engage in preventive health activities and a self-management of their genetic and biological propensity to develop a disease. Such engagement ranges from monitoring blood glucose levels with small, portable devices to the use of full-body, comprehensive physical, mental and emotional self-tracking technologies. The key objective of patient empowerment is the right and responsibility of patients to access health information and to make their own health related decisions using their own data. This is an extension of precision and personalized medicine, whereby patients are not just receivers of data and knowledge by their carers, but rather they become actively engaged in the production, analysis and interpretation of such data and knowledge. The pursuit of quantifying one’s self can have several benefits including learning how to live with a disease while improving one’s understanding of how to make behavioral changes that can improve their physical, mental, and emotional health. Research has shown that self-tracking technologies are widely used in people’s daily lives and health care to promote health and well-being.
However, there are also risks associated with quantified self-projects. Some critics argue that the use of self-tracking devices can promote extreme forms of healthism and individualism. For example, the billionaire entrepreneur Bryan Johnson has developed a so-called blueprint with a team of 30 doctors to improve his physical and mental performance. According to his website, he spent two years and millions of dollars developing an algorithm that takes better care of him than he can himself. The blueprint incorporates, not just a daily nutrition and supplement routine, but also a series of weekly and monthly tests, including ultrasounds, colonoscopies, MRI scans and blood tests to empower him to make better decisions about his health and wellbeing.
Some critics have raised concerns about the extreme measures taken by Johnson and the potential risks associated with such an approach, including the high costs of following the blueprint, but also the potential for harm from unproven treatments and the ethical implications of such extreme measures. Some have argued that the techno-utopian discourses concerning the possibilities afforded by self-tracking technologies do not acknowledge the complexities and ambivalences that are part of self-monitoring health, both for patients and for healthcare providers. These include “the emotions and resistances they provoke, their contribution to the burden of self-care and the invisible work on the part of healthcare workers that they require to operate”. Empowerment should be understood as both a process and an outcome and involves a patient’s interaction with other patients suffering from similar conditions, but also with doctors, and other ecosystem actors.
Indeed, patient empowerment has disrupted the role of many ecosystem actors in healthcare service provision and management. It has put more pressure for healthcare providers such as hospitals and their specialized experts including doctors to become more digitally augmented. Doctors are no longer practicing medicine, they have become part of a team of multidisciplinary experts including data scientists, molecular biologists, and technology engineers. This team has greater expertise to implement more targeted plans for personalized medicine in comparison to single doctors without digital technologies. Together with this multidisciplinary team, doctors are in a better position to make informed decisions about how patients should interpret data about their disease. This is paramount in avoiding some of the risks mentioned above in relation to self-tracking devices for better monitoring one’s health. These technologies are important and critical for helping patients – especially those suffering from chronic diseases – to receive remote, on-demand care round the clock.
However, to achieve this, doctors and other carers need to be trained on how to use those technologies themselves, as well as to be supported by technology experts that can help them interpret data generated from those technologies. Evidently, the move towards preventive, personalized medicine has empowered indidviuals to become mor eactive in their health and wellbeing. Such empowerment has also generated new challenges but also transformative opportunities on healthcare ecosystems.